Dr. Sanoop Kumar Sherin Sabu
Sarcopenia assessment is very important in chronic liver disease (CLD) and bedridden patients because it has direct clinical, prognostic, and management implications.
1. In Chronic Liver Disease (CLD)
Why sarcopenia matters:
- High prevalence
- Up to 40–70% of cirrhotic patients have sarcopenia.
- Predicts poor outcomes
- Increased risk of complications: infections, hepatic encephalopathy, ascites.
- Higher mortality on transplant waitlist.
- Poor post-transplant outcomes if sarcopenic.
- Impaired liver function & metabolism
- Low muscle mass → decreased ammonia detoxification, worsening encephalopathy.
- Protein-energy malnutrition accelerates muscle loss and frailty.
- Guides management
- Nutritional intervention: high-protein diet, branched-chain amino acids.
- Physical therapy to improve muscle mass before transplant.
Summary: Sarcopenia in CLD is a strong prognostic marker and helps tailor nutrition and exercise interventions.
2. In Bedridden / Immobilized Patients
Why sarcopenia matters:
- Rapid muscle loss
- Muscle mass decreases ~1–2% per day of immobilization.
- Functional decline
- Reduced strength → difficulty with ADLs, higher dependency.
- Increased risk of falls and pressure sores.
- Complications
- Immobility + sarcopenia → higher infection risk, delayed recovery.
- Prolonged hospitalization → further deconditioning.
- Intervention guidance
- Early rehabilitation / physiotherapy prevents further loss.
- Nutritional supplementation (protein, vitamin D, amino acids) improves outcomes.
Summary: Early detection of sarcopenia in bedridden patients can prevent functional decline, reduce complications, and shorten hospital stay.
Clinical Examinations to Suspect Sarcopenia and Frailty
| Test | Normal (Male) | Normal (Female) | How to test (short) |
| Hand grip strength | ≥ 27 kg | ≥ 16 kg | Squeeze dynamometer with dominant hand, best of 3 |
| Chair stand test (5× sit-to-stand) | ≤ 15 sec | ≤ 15 sec | Stand up & sit down 5 times without using arms |
| Gait speed (4 m walk) | ≥ 0.8 m/s Will walk 4 meter in less than 5 seconds | ≥ 0.8 m/s Will walk 4 meter in less than 5 seconds | Walk 4 m at usual pace, time with stopwatch |
These are often enough to suspect sarcopenia clinically.

Dynamometer
Investigations to Prove
1.DEXA SCAN
Normal Values for Muscle Mass
| Measurement | Male (Normal) | Female (Normal) | Notes |
| Appendicular Skeletal Muscle Mass (ASM, kg) | ≥ 20 kg | ≥ 15 kg | ASM = sum of lean mass in arms + legs |
| ASM / height² (kg/m²) | ≥ 7.0 kg/m² | ≥ 5.5 kg/m² | Used in EWGSOP2 / AWGS criteria (Ref 1) |
| Skeletal Muscle Index (SMI, via BIA) | ≥ 7.0 kg/m² | ≥ 5.7 kg/m² | Similar to ASM/height²; slightly different cut-offs by region |
| Lean mass % (total body) | ~75% | ~65% | Approximate; varies by age & ethnicity |
Guideline based Interpretation (EWGSOP2 guidelines)
- Probable sarcopenia: Low muscle strength (grip strength or chair rise)
- Confirmed sarcopenia: Low muscle mass (ASM / height² below cut-off)
- Severe sarcopenia: Low muscle mass + low strength + low physical performance (e.g., gait speed <0.8 m/s)
2. Muscle Mass Assessment at L3 Vertebra (CT scan)
What is measured: (Ref 2)
- Cross-sectional area (CSA) of skeletal muscles at the third lumbar vertebra (L3)
- Muscles included: psoas, erector spinae, quadratus lumborum, abdominal wall muscles
Why L3:
- Muscle area at L3 correlates strongly with whole-body muscle mass
Normal / Cut-off Values
| Sex | Skeletal Muscle Index (SMI) at L3 SMI = muscle CSA at L3 / height² |
| Male | ≥ 52.4 cm²/m² |
| Female | ≥ 38.5 cm²/m² |
Interpretation:
- Below cut-off → sarcopenia
Utility of L3-CT
- L3 CT gives precise, reproducible muscle mass assessment
- Often used in oncology, geriatrics, ICU patients
- Advantage: can use routine abdominal CT scans without extra radiation
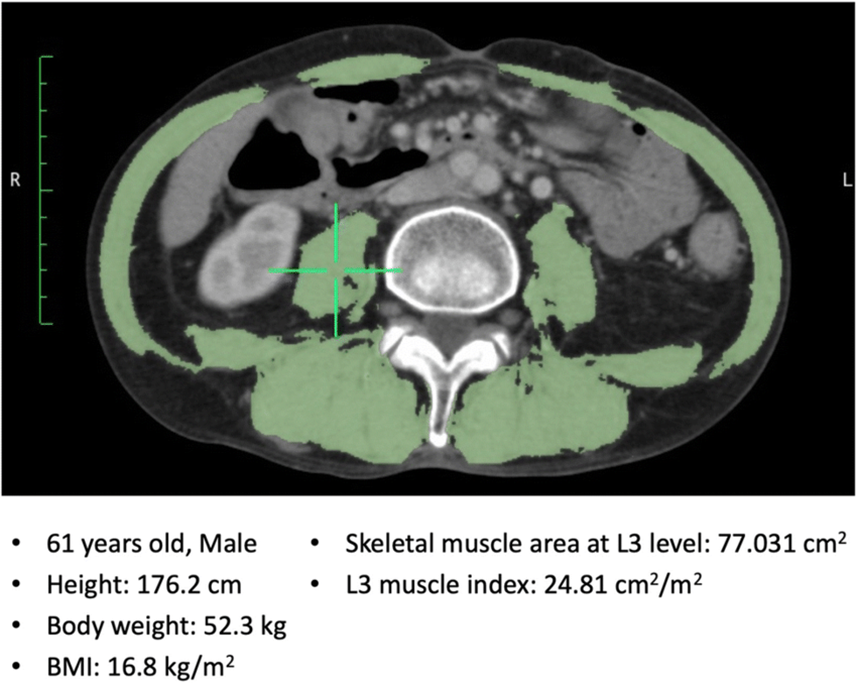
Representative image of the skeletal muscle area at the L3 level. The skeletal muscle area was 77.031 cm² and L3 muscle index was 24.81 cm²/m². BMI body mass index, L3 the third lumbar vertebra. (Adapted from Ref 3)
3. CT Muscle Density (Hounsfield Units, HU) – L3 Vertebra
What it measures: (Ref 2)
- Skeletal muscle radiodensity in HU
- High HU → lean, healthy muscle
- Low HU → fat infiltration (myosteatosis / poor muscle quality)
| Sex | HU Cut-off for Low Muscle Quality | Notes |
| Male | < 41 HU | Indicates myosteatosis / poor muscle quality |
| Female | < 33 HU | Fatty infiltration of muscle |
References
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31. doi: 10.1093/ageing/afy169. Erratum in: Age Ageing. 2019 Jul 1;48(4):601. doi: 10.1093/ageing/afz046. PMID: 30312372; PMCID: PMC6322506.
- Derstine BA, Holcombe SA, Ross BE, Wang NC, Su GL, Wang SC. Skeletal muscle cutoff values for sarcopenia diagnosis using T10 to L5 measurements in a healthy US population. Sci Rep. 2018 Jul 27;8(1):11369. doi: 10.1038/s41598-018-29825-5. PMID: 30054580; PMCID: PMC6063941.
- Clinical impact of skeletal muscle area in patients with non-small cell lung cancer treated with anti-PD-1 inhibitors – Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/figure/Representative-image-of-the-skeletal-muscle-area-at-the-L3-level-The-skeletal-muscle_fig1_339059671